
I had a meniscal transplant operation last May by Mr Ian McDermott and I cannot thank Mr McDermott enough.
Many years ago I had my cartilage removed in my left knee and over the years with bone on bone rubbing against each other it left me in pain with restrictive movement so I had had micro fracturing which had been successful for four years. However with the life expectancy of this operation up I endured many months of not being able to sleep due to the constant pain in my knee which was not relieved by pain killers. My cycling had to stop and I had even got to the stage of only being able to walk very short distances (less than half a mile) before I would have to sit down in agony.
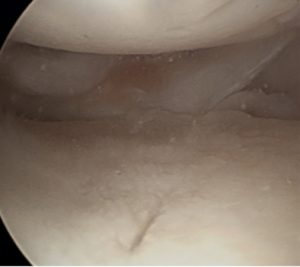
Sharon’s medial compartment of her knee, with a completely missing (previously excised elsewhere) medial meniscus, and with progressive articular cartilage damage developing (early degeneration / arthritis)
After a consultation with Mr McDermott I was offered a meniscal transplant operation. I had the operation at London Bridge hospital where everything went to plan, the only issue being I live in the Isle of Man and with not being able to fly for three months it meant a car journey up to Liverpool followed by a boat journey. The initial recovery was to protect the transplant for 6 weeks and give it chance to take so I was in a knee brace to keep the leg in a straight position with non to minimal weight bearing. After two weeks I had to go back to London for a check-up and have the stitches removed and everything was looking good.
Once the six weeks were up I was able to discard the knee brace and start physio. The initial targets were to get the bend back in my knee and start to put my weight through my leg. As well as regular physio to help get the bend back I also used a static exercise bike, initially only being able to complete a partial revolution to help with this. Gradually over the following six months I was able to increase the intensity of the exercise and I noticed a significant improvement after Christmas. I was able to start to get back out on both my mountain and road bikes and walking both great passions of mine. These activities are something that I had not been able to do for over 18 months and I must admit it has made me really appreciate the simple things in life.
The excruciating pain in my knee has now gone and the only pain I get is a stinging sensation from time to time which does not cause me any issues.
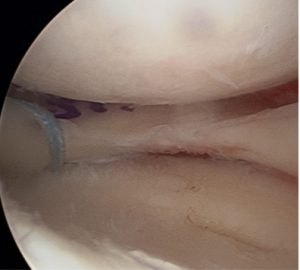
Sharon’s medial compartment at the end of the meniscal transplantation procedure, with a new medial meniscus inserted in the knee.
I would thoroughly recommend this operation to anyone and the best advice I could give is be patient. I was told the recovery was a good nine months and this was the case but I have gone from not being able to sleep due to constant pain to being virtually pain free and able to walk on a daily basis along with cycling three times a week, something I would never have been able to do 18 months ago.



