
What is ‘pie-crusting the MCL’?
Quite often, when I’m doing an arthroscopy and looking for a probable medial meniscal tear, the medial compartment can be a bit tight, in which case it can be difficult to see the posterior horn of the medial meniscus, and difficult to get to it (particularly without scuffing and damaging the articular cartilage on the surface of the medial femoral condyle).
If, at arthroscopy, the medial compartment is tight, and if visualisation is limited, and if I have any suspicion that there might actually be an issue with the posterior horn of the medial meniscus, then I have a very low threshold for proceeding with pie-crusting the MCL.
Pie-crusting the MCL involves poking a needle through the skin at the medial side of the knee, level with the medial joint line and just more than half of the way back, from front to back, and then perforating the MCL and the posterior oblique ligament on the medial side of the knee with multiple tiny punctures with the needle, whilst holding the MCL under tension by applying a valgus stress to the knee. With this, the MCL ‘gives’, with what is effectively a minor partial tear: as the MCL releases, the medial compartment opens up, and one can then see the whole of the posterior horn of the medial meniscus far more clearly, and one can access the meniscus much more easily.
The pie-crusted MCL heals up absolutely fine within just a few weeks, exactly the same as a minor traumatic MCL sprain does, and there is good quality published research that shows that pie-crusting the MCL does not result in any ongoing symptoms or laxity in the knee, once the patient has done their standard rehab. Pie-crusting the MCL can cause a bit of increased pain and bruising around the medial side of the knee, but this rarely ever affects or delays the patient’s rehab and overall recovery.
I routinely pie-crust the MCL for most of the medial meniscal repairs that I do, and for every case when I’m performing meniscal replacement surgery, by meniscal allograft transplantation.
CASE EXAMPLE
A 30-year-old gentleman presented with a couple of months’ history of pain around the medial side of his right knee, after having twisted the knee. The patient had actually had 2 x previous arthroscopies of that same knee in the past, several years ago (performed elsewhere), also for medial meniscal tears: with the first op, the meniscus had apparently been trimmed, and with the second arthroscopy, apparently a repair had been performed, and both operations had been ‘successful’.
The patient had medial joint line pain, pain medially with deep flexion, and a positive McMurray’s test. His MRI scan showed that his medial meniscus was slightly reduced in volume, from the previous meniscal trim, and the meniscal remnant was torn.
The patient’s symptoms were not improving with time, and the patient felt that his knee symptoms and functional restrictions were bad enough to justify taking things further, with another arthroscopy of his knee.
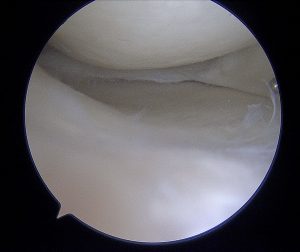
We proceeded with an arthroscopy, and the initial appearances of the medial compartment were thus:
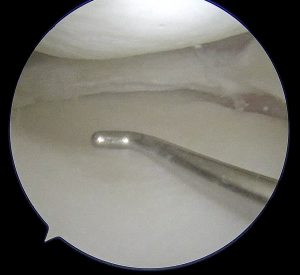
The MCL was pie-crusted and partially released, which then gave the following view:
Now, when the posterior horn remnant of the medial meniscus could be seen clearly and reached and probed property, this revealed that the meniscal tissue was actually severely torn, with a large, complex, unstable tear:

A further partial meniscectomy was performed, which cured the patient’s symptoms.
Importantly, this severe tear would most probably have been completely missed if a surgeon had performed an arthroscopy of this patient’s knee without them actually having pie-crusted the MCL, to gain sufficient visualisation and access!
So, if you’re a patient or a physio, and if you were curious about what ‘pie-crusting the MLC’ meant, and why a surgeon might do it, then hopefully now this is clear.
And if you’re a younger knee surgeon, then: “Think pie-crusting? DO pie-crusting!” – I’ve never pie-crusted an MCL and regretted it, but I’m pretty sure that there are a lot of patients out there who’ve had arthroscopies of their knees for suspected medial meniscal tears, who’ve not had their MCL pie-crusted, and who, as a result, ended up having their tear either missed or inadequately trimmed, or who possibly ended up with unnecessary damage to the articular cartilage on the surface of their medial femoral condyle, as their surgeon struggled to adequately reach the back of their medial compartment with meniscal punches, shavers etc.
READ MORE…. https://www.arthroscopyjournal.org/article/S0749-8063(20)30331-5/fulltext