
#treatment
Meniscal transplantation
- Loss of a meniscus tends to lead to arthritis in a knee.
- If a patient has lost most of or even the entire meniscus and if they are getting problems as a result of this then the meniscus can be replaced by surgically implanting a completely new meniscus from a donor. This is called meniscal allograft transplantation.
- There are very few surgeons indeed in the UK who actually specialise in meniscal transplantation. The surgery is highly complex and should only really be undertaken by specialist surgeons with specific training and experience.
- The meniscal allograft (donor meniscus) comes from a registered Tissue Bank. The grafts are sized, sterilized and deep frozen. There are no living cells in the tissue, and the graft acts as a biological scaffold. The patient’s cells grow into the graft to give a living meniscus, which becomes the patient’s own tissue.
- There are no issues with rejection at all, and tissue typing or immunosuppressive drugs are not required.
- The risk of a donor graft being infected is tiny, as is apparently less than 1 in 1.6million.
- The rehab after meniscal transplantation is very slow.
- Meniscal transplantation has been shown to decrease patients’ knee pain, increase their function and keep their knees going for longer, delaying the time when a knee replacement might potentially become necessary.
- The success rate for meniscal transplantation is about 85%.
Read more...
Meniscal transplantation is not new – the first reported series of human meniscal transplants was reported back in 1989 by Milachowski, in Germany. Meniscal transplantation is not ‘experimental’ – there are hundreds of scientific articles published about the subject, with numerous studies reporting the short and long-term clinical results. However, meniscal transplantation is a complicated subject and the surgery itself is very difficult and technically demanding. There is only a small handful of knee surgeons in the UK with proper experience in this procedure, and meniscal transplantation should only be undertaken by specialist knee surgeons with a particular sub-specialist interest in this area.
The menisci are important load sharers and shock absorbers in the knee, and unfortunately meniscal tears are very common. Most meniscal tears are not repairable (CLICK HERE for information about meniscal repair), and if they are symptomatic enough then they are likely to end up needing surgical trimming – a partial or total meniscectomy (CLICK HERE for information about meniscal trimming).
The risk of subsequently developing arthritis in that part of the knee where a meniscus has previously been removed is increased by about x15, when viewed about 20 years later. If a patient does go on to develop increasing symptoms and signs of early arthritis in their knee after a previous meniscectomy then meniscal replacement surgery might be indicated.
If only part of the meniscus has been removed but the peripheral rim is still fully intact all the way round, then the patient might be suitable for an artificial bioabsorbable meniscal scaffold (CLICK HERE for information about meniscal scaffolds). However, if the whole meniscus is missing or if there is any discontinuity in the meniscal rim, then the patient is likely to need meniscal transplantation.
What is an allograft?
Meniscal allografts are whole intact meniscal cartilages harvested from donors. The donors are people such as patients on ITU who have unfortunately suffered brain death from, for example, car accidents, and whose family wish their organs to be donated. When the transplant retrieval teams harvest organs such as the heart or the kidneys, they also take other important tissue such as corneas, bone and tendons. The meniscal cartilages can also be harvested.
A meniscal allograft from a donor, sized to match the patient’s knee. The graft is provided deep frozen and it is then thawed in theatre prior to use. The graft is then prepared by the surgeon prior to implantation into the knee.
What are the risks of infection?
The donors are very carefully screened for any high risk categories for infection. The donor’s blood is tested carefully for bacteria, viruses or fungi. The meniscal tissue is harvested in a sterile way, like an operation, and the tissue itself is swabbed and tested for any infectious agents. If any of the above tests come back as positive then the graft tissue is discarded and not used. The tissue is then sterilized (by chemical sterilization) and then deep frozen and stored in a EU Directive compliant registered Tissue Bank.
It has been estimated that the risk of disease transmission (contamination) in a graft is less than 1 in 1.6million.
What about tissue typing?
There are no living cells within a meniscal allograft (not like a living organ like a kidney transplant), and the small amount of cellular material that does remain within the tissue is locked deep in the cartilage matrix, inaccessible to your immune system. Therefore, meniscal allografts do not illicit an immune response, you do not need to test and match tissue types, anyone can have anyone else’s meniscus implanted, and there is no need for any nasty immunosuppressive drugs or steroids.
What about size matching?
What is important with a meniscal allograft is that the size of the graft is matched carefully to the size of the patient receiving the graft. There are various methods available for size matching grafts, but probably the best is to rely on simple X-rays with size markers attached, so that the dimensions of the tibial plateau can be measured accurately, and the appropriate sized meniscal allograft from the Tissue Bank store can then be chosen.
The operation
Meniscal transplantation is a technically challenging procedure. There are a number of different surgical techniques described, with quite wide variation in fixation methods. It is vital that the anterior and posterior insertional ligaments are fixed solidly and securely down to the bone of the tibial plateau, and the peripheral rim of the meniscus is then stitched to the inside lining (the capsule) of the knee. The operation takes about 2+ hours, under a general anaesthetic, although it can take significantly longer than this if the operation is combined with other concomitant procedures, such as anterior cruciate ligament reconstruction and/or articular cartilage grafting. The operation is normally performed with a 1-night post-operative stay in hospital, and most patients are ready to go home the morning after the operation.
Meniscal allograft being prepared.
Meniscal allograft being prepared.
Patient with a completely missing
medial meniscus, from a previous
meniscal tear that was trimmed with
a total meniscectomy.
Meniscal allograft surgically
implanted into the knee and fixed to
the bone of the tibia at the front and
back, and then stitched to the
capsule of the knee around the
peripheral edge.
The rehab
The rehab after meniscal transplantation is critical. In the early stages it is important to protect the knee, to allow the meniscal allograft to heal into place. I therefore normally keep my patients minimal (toe touch) partial weight bearing with 2 crutches for the first 6 weeks, with the knee in a hinged brace locked to prevent deep knee flexion. After 6 weeks patients start regular intensive physio rehab treatments (seeing their physio ideally 3 times a week to start with), focusing on regaining the full range of motion in the joint, building up towards full weight bearing ASAP and starting to regain some muscle strength and bulk plus starting to retrain the proprioceptive reflexes. As soon as the knee is good enough, patients start non-impact, non-twisting exercises such as the exercise bike. However, it does take a number of months for the allograft to bully bed in and mature, and therefore for the 1st 9 months I advise patient to avoid any deep loaded squats, lunges, heavy weights, loaded twisting/pivoting or any kind of impact (running, jumping etc).
The results
The results of meniscal transplantation are very good, but not perfect and not guaranteed. Nothing is as good as your own natural original meniscus, and also by the time that most patients come to see me seeking possible meniscal transplantation they’ve normally got other damage in the knee (such as ligament tears) and/or already begun to develop articular cartilage damage, with wear and tear / early degenerative changes.
Overall, 85% of patients achieve a good or excellent outcome after meniscal transplantation (when reviewed at 5-year follow-up). If meniscal transplantation is performed in more severely damaged knees, along with other surgical procedures such as ligament reconstruction or articular cartilage transplantation, then the likely anticipated outcomes tend to be lower. However, this is very much salvage surgery, for patients with badly damaged knees and severe symptoms, who need something doing but who are too young for a knee replacement.
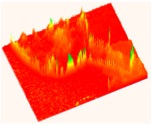
Pressure profiles in the lateral
compartment of a knee with
the lateral meniscus intact.
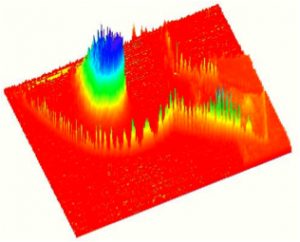
Pressure profile with the
lateral meniscus removed:
the contact surface area
is decreased and the peak
contact pressures increase
very significantly.
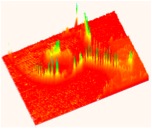
Pressure profile in the same
knee after lateral meniscal
transplantation has been
performed: the peak contact
pressures are reduced back
towards normal.

Pressure measured in MPa
Case studies
CLICK HERE to read Sharon Nicholson’s experience of undergoing Meniscal Transplantation.
CLICK HERE to read Sarah Conway’s personal experience of Meniscal Transplantation.
CLICK HERE to read Louise Ayling’s account of undergoing combined Revision ACL Reconstruction + Meniscal Transplantation

Written by
Mr Ian McDermott
Consultant Knee Surgeon
London
www.kneesurgeon.london
Last updated 19-3-17