
#treatment
Meniscal repair
- Only about 25% of meniscal tears are actually repairable.
- Not all orthopaedic surgeons can actually manage meniscal repair, so you must choose your surgeon very carefully.
- The tears that are repairable tend to be in younger patients (<40) with fresher, more recent traumatic tears, eg from a sports injury.
- The longer a meniscal tear is left, the less likely it is that it will actually be repairable.
- Ragged, complex, degenerative tears in older patients are generally not repairable.
- The success rate for meniscal repairs healing up is about 90%.
- The rehab and recovery after meniscal repair is slower than it is after just a meniscal trim (partial meniscectomy).
Read more
The menisci are important load sharers and shock absorbers in the knee, and if they tear then they can cause significant symptoms in the joint. If a patient has a meniscal cartilage tear and their symptoms are significant enough to justify it, then they are likely to end needing a knee arthroscopy. Unfortunately, one can rarely accurately or confidently predict from an MRI scan whether any particular meniscal tear is going to be repairable or not, and this can only actually be determined intra-operatively, at the time of the actual knee arthroscopy, when the meniscal tissue and the tear are visualized carefully, inspected and probed.
If at arthroscopy a meniscal tear is found to be repairable then your surgeon will go ahead directly and repair the tissue, by stitching it back together. Otherwise, if a meniscal tear is not repairable then the torn tissue will be trimmed back to a smooth stable surface, but trying to leave behind in place as much tissue as possible.
The more meniscal tissue is lost, the less of a shock absorber is left in the knee, and therefore the more wear and tear is likely to develop with time, and the bigger the long term risk of arthritis in the joint (with pain, swelling, stiffness and immobility, eventually leading to a need for joint replacement surgery). Therefore, if a tear appears to be repairable and likely to have a good chance of healing up successfully then it should be repaired.
Sadly, not all surgeons are either well-practiced and good at meniscal repair, and some surgeons do not even perform meniscal repair at all, but instead simply chop out all meniscal tears! Therefore, if you care about the long-term well-being of your knee then it is essential that you actually check out your surgeon before committing to any surgery, to be sure whether or not they do/can actually perform meniscal repair, and whether or not this is something that they perform regularly.
Unfortunately, only a minority of meniscal tears are actually repairable. The repair rate often quoted in the literature is about 10 to 15%. My personal repair rate is about 25% — each surgeon’s threshold for attempting meniscal repair will vary according to their experience and confidence in their techniques.
Which tears are likely to be repairable?
Tears that have a relatively better likelihood of being repairable are:-
- Tears in younger patients (<40)
- Fresh, acute tears
- Vertical peripheral circumferential tears
- Partial thickness tears
- Some horizontal cleavage tears
- Some bucket handle tears, if caught early
The kind of tears that tend not to be repairable are:-
- Ragged degenerate tears
- Tears in older patients
- Chronic tears that have been there a long time
- Radial tears (although some radial tears in children can be repaired)
- Tears in the avascular inner free margin of the meniscus
- Why are so many tears not repairable?
Meniscal tissue has a poor blood supply, and only about the outer peripheral third of the tissue actually has a decent blood supply (the ‘red zone’). The inner 2/3 has no blood supply, and is called the avascular or ‘white’ zone. Tears in the red zone might heal (very occasionally on their own, without surgery, but more likely after a meniscal repair). Tears in the inner whilte zone won’t heal. Tears at the red-white zone junction might heal, if they are repaired well, if the meniscal tissue is in good enough condition (not degenerate) and if supplementary techniques such as trephining are employed (where the meniscal tissue is punctured with small holes to promote bleeding into the tissue via vascular access channels, to encourage healing).
So, as a general rule for healing of meniscal tears (repairs):-
- red-red will,
- white-white won’t,
- red-white might!
How is a meniscal repair performed?
There are various different techniques that can be employed for repairing a torn meniscus.
In the old days, the only way to repair a meniscal tear was to put stitches into the meniscus from the front of the knee via open surgery, and the knots would be tied around the back of the knee, behind the capsule. The back of the knee is where all the important major blood vessels and nerves are, and is an extremely dangerous area (sometimes referred to in surgical circles as ‘tiger territory’). One cannot make small incisions round the back of the knee, for fear of causing serious nerve of blood vessel damage. Therefore, open ‘inside-out’ meniscal repair requires fairly large incisions around the back of the knee so that you can see where the needles are going and where the knots can safely be tied. This leaves large nasty scars around the back of the knee, which is an awkward and sensitive area, and there is still a significant percentage risk of complications with neurovascular damage.
Over the years, people have tried to develop various different better ways of repairing the menisci, particularly repairing meniscal tears arthroscopically, ‘through the keyhole’, rather than with open surgery.
A few years ago various companies developed ‘all-inside’ meniscal repair techniques using ‘bioabsorbable’ darts and arrows that could be fired across a meniscal tear arthroscopically. This was much easier and quicker to perform than an open ‘inside-out’ meniscal repair. However, personally, I would never use any of these devices, for a number of very good reasons:-
- The arrows/darts are made of very hard solid material that is like hard plastic. Although the material does, allegedly, slowly dissolve within the body, this takes absolutely ages, and until that point the dart/arrow remains hard, sharp and dangerous!
- There are case reports of the hard ends of arrows/darts protruding out of the meniscal surface into the knee joint, and gouging great chunks of articular cartilage out of the surface of the femoral condyle with knee movements, causing severe joint damage.
- There are reports of arrows/darts breaking inside the knee, and floating around as loose bodies.
- There are reports of arrows/darts perforating backwards too far and causing neurovascular damage.
- There are reports of arrows/darts migrating in the soft tissues and causing problems.
In my opinion, the very best kit for repairing a meniscal tear is to use some of the newest all-inside arthroscopic repair devices that have tiny suture anchors loaded into small slotted needles, with sutures that have slip knots that can be tightened easily and securely. In my hands, the best devices available are the Smith and Newphew Fast-Fix-360 sutures and the Stryker Air meniscal sutures.
Smith & Nephew Fast-FIx-360
The Smith & Nephew Fast-Fix 360 is the latest generation of meniscal repair devices produced by Smith & Nephew, who have a long history of producing some of the very best surgical equipment for arthroscopic knee surgery.
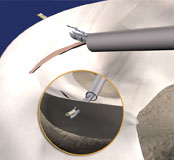
The delivery needle is passed through the meniscus and an anchor is lodged behind the meniscal rim, with a suture attached.
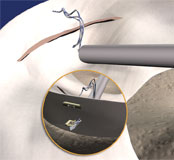
A second anchor is then placed through the meniscus, the other side of the meniscal tear, and this also has a suture attached to it.
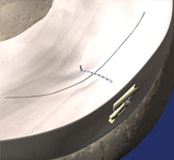
The sutures are pulled and the slip knot is pushed, which tightens up the meniscal stitch, and the meniscal suture end is then cut.
Stryker Air meniscal sutures
What is the rehab after a meniscal repair?
CLICK HERE for detailed information about what rehab is required after a meniscal repair.
The results of meniscal repair
The best success rate that can be anticipated after meniscal repair is about 90%. This means that if appropriate rehab advice is followed properly, then about 90% of meniscal repairs will heal up successfully, which means that the patient then has a normal, fully functional meniscus again, and no increased long-term risk of arthritis in that knee. However, this also means that about 10% of meniscal repairs don’t heal up successfully.
How do you know that a meniscal tear has actually healed up?
After a meniscal repair, the first 6-week period is all about protecting the knee. The 2nd 6-week period is about carefully getting the knee going, with regular physio rehab. By 3 months, hopefully the meniscal repair has healed up and is sufficient strong to allow patients to start gradually getting back to full normal activities.
At the 3-month post-op mark, you would ideally want to know that the meniscal repair has actually healed prior to trying to get back to normal. However, there is no point in getting an MRI scan to check this, as on an MRI scan you are likely to see a white line in the meniscus, but you won’t know whether this is scar tissue from where the repair has healed successfully, whether this represents swelling or degeneration, whether the repair has failed to heal, or it could even simply be the meniscus stitch itself. One could simply perform a repeat arthroscopy, to look inside the knee and probe the meniscus and check directly whether or not the tear has actually healed. However, as about 90% of meniscal tears do heal up successfully, that would mean that 9 out of 10 of these repeat arthroscopies would not only be unnecessary, but they would also subject the patient to additional pain, hassle and risk (risks from another operation and another anaesthetic), and delay the patient’s actual recovery, and this really cannot be justified. Therefore, the only practical and appropriate way to find out whether a meniscal tear has healed is to simply gradually stress test the knee and see how things go … if the knee does well and feels good then the repair has healed. If not, and if the patient has residual symptoms in their knee then one must assume that the repair has failed to heal.
What if a meniscal repair fails to heal?
In the 10% failure group after meniscal repair, the patient can then be faced with a difficult decision about their knee. If any potential ongoing symptoms are only minimal and manageable then there is a good argument for simply leaving things alone and avoiding any further surgery. However, if a knee is still causing significant pain or functional restriction after an unsuccessful attempt at meniscal repair then it might be necessary to perform a repeat arthroscopy to re-check the meniscus: if a residual tear is actually found then it is very rare for a surgeon to attempt another, 2nd attempt at meniscal repair if the 1st previous attempt has failed, and it is very likely the meniscus will simply have to be trimmed. No-one wants a patient to have to have 2 knee ops rather than just one. Therefore, it is essential that each surgeon picks and chooses very carefully which meniscal tears to repair and which to trim, and this is a judgment call that can only be made intra-operatively, at the time of the actual surgery, based on the quality of the meniscal tissue, the morphology and location of the tear, the blood supply to the tissue, the stability of the tear and the age and expectations of the patient.
The importance of proper pre-op counseling…
This is why proper, detailed pre-operative discussion/counseling is so very important, because as a surgeon I need to know what the patient’s preferences are for repair vs trimming, because when I’m in there inside the knee the patient is asleep. Therefore, before any arthroscopy for a potential meniscal repair, it is vital that your surgeon discusses with you the various options available, the rough % probability of your tear potentially being repairable in their hands, the potential risks, the rehab that might be required, and the potential success rates.
The importance of picking the right surgeon for your arthroscopy...
If you’re young and you’ve got a meniscal tear, and if you care about your knee, then you must check out your surgeon prior to letting them operate on your knee, and you must check:-
- Are they actually a specialist knee surgeon, or just a generalist orthopaedic surgeon?
- Can they actually do a meniscal repair?
- How many meniscal repairs do they do?
- What are their success rates?
- Do they include you in the decision-making process about what potentially might be done to your knee?
- Have you been given sufficient information about everything?
Case Study
CLICK HERE to read ‘My Meniscal Repair’ by Laura Procter, about her experiences of undergoing meniscal repair surgery.

Written by
Mr Ian McDermott
Consultant Knee Surgeon
London
www.kneesurgeon.london
Last updated 7th March 2021