
#condition
Ramp lesions
A ramp lesion is a tear around the periphery of the posterior horn of the medial meniscus, with a detachment of the meniscus from the posterior capsule (a tear of the meniscotibial ligament).
Ramp lesions were first described by Strobel, back in 1988. Ramp lesions normally occur specifically in association with ACL tears, and it has been estimated that ramp lesions may actually occur in up to 17% of all ACL tears.
Ramp lesions are often missed on MRI and they can also easily be missed intra-operatively, unless the posterior horn of the meniscus is inspected and probed very carefully.
Most ramp lesions are, however, surgically repairable.
What is a ramp lesion?
The meniscal cartilages are two crescent-shaped wedges of elastic cartilage in the knee that act as important ‘shock absorbers’ / load sharers within the joint. [READ MORE] The medial meniscus is less mobile than the lateral meniscus, and in particular, the posterior horn (the back part) of the medial meniscus undergoes significant compressive forces when the knee is in deep flexion, combined with shear forces when one twists on a loaded knee with the knee bent.
The medial meniscus is attached to the bone of the top surface of the tibia at the front and the back by very strong ‘insertional ligaments’. However, it is also attached to the tibia around the periphery of its circumference by ‘the meniscotibial ligament’ (a.k.a. the coronary ligament).
A ‘ramp lesion’ is where the back part of the meniscotibial ligament tears around the periphery of the posterior horn of the medial meniscus. This tends to happen most frequently in association with tears of the ACL, where a loaded knee is forced into external rotation and valgus (bent sideway to the outer side) whilst the joint is in a flexed (bent) position. It has been estimated that ramp lesions may actually occur in up to 17% of all ACL tears.
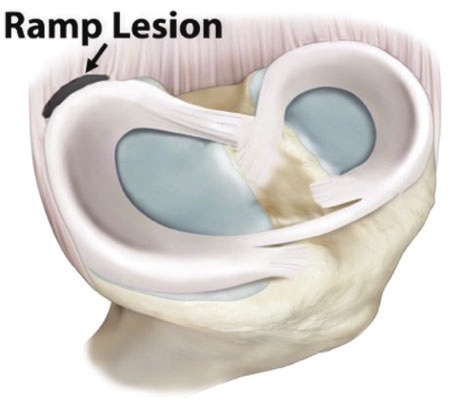
A ramp lesion is a tear of the meniscotibial ligament at the back of the medial meniscus.
Symptoms of a ramp lesion
The meniscus has nerve fibres in it, and most of these nerve fibres are found towards the periphery of the meniscus, where the blood supply is. This is exactly the area affected by a ramp lesion. Hence, ramp lesions tend to cause pain in the knee particularly around the inner/back (posteromedial) or fully round the back of the joint when this area of the meniscus is loaded – i.e. with deep flexion of the joint or with loaded twisting on a bent knee.
Cadaveric studies have shown that ramp lesions affect the biomechanics of the knee, and can lead to increased anterior and external rotatory laxity of the joint. This is of particular relevance in the ACL-deficient knee.
Imaging of ramp lesions
MRI is reasonably good (about 90% accurate) at diagnosing meniscal tears in general. However, ramp lesions can be particularly difficult to see on MRI, as the meniscotibial ligament is small and poor visualised. Imaging therefore frequently misses ramp lesions.
In one study, MRI was shown to pick up 77% of ramp lesions (i.e. it missed 23%). However, in another study, MRI missed all of the ramp lesions that were subsequently confirmed at the time of arthroscopy!
Sometimes, MRI may show a thin slither of fluid just posterior to the posterior horn of the medial meniscus, which can often represent a meniscotibial ligament tear. Another sign that can be of particular value is the presence of bone bruising with the posterior aspect of the proximal tibial plateau, just underneath the posterior horn of the medial meniscus, which is an indirect sign of a probable ramp lesion.
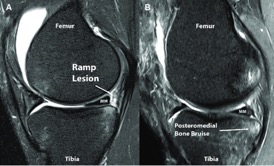
MRI signs of a ramp lesion.
Should a ramp lesion be repaired?
If a ramp lesion is asymptomatic and not causing the patient any actual functional limitations, then there is reasonable argument for potentially just leaving it alone.
However, most ramp lesions tend to be confirmed at the time of surgery, which is usually as part of a surgical ACL reconstruction. If a ramp lesion is found intra-operatively, then there is a strong argument for going ahead and performing a surgical meniscal repair, then and there, as surgical repair has a very good success rate. Most surgeons agree that this gives the patient the best possible chance of doing well from their ACL surgery (in the long term as well as the short term), and it reduces the likelihood of the patient ending up needing further surgery (to go back in later and potentially deal with a residual ramp lesion) later, as an additional subsequent operation.
How to detect a ramp lesion
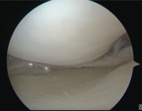
Access to the posterior aspect of the medial compartment can often be tight and restricted, making clear visualisation difficult. However, even when visualisation is poor, it is nearly always possible to pass an arthroscopic probe under the posterior horn of the medial meniscus. If the posterior meniscocapsular attachment is intact, then the probe hits a firm stop and the hook cannot be rotated up (proximally) behind the bulk of the tissue of the meniscal posterior horn. If, however, there is a ramp lesion present, then the tip of the probe can be rotated and passed posterior to the posterior horn, ‘catching’ the posterior horn as one pulls anteriorly. Therefore, even if a ramp lesion cannot be visualised from the front of the knee via standard portals, it can be felt.

Arthroscopic probe passing into a ramp lesion on the under-surface of the posterior horn of the medial meniscus, with the tip of the probe going into the tear and hooking the posterior horn tissue.
If there is any suspicion of a ramp lesion but if visualisation and access are actually restricted, then one should have a very low threshold for proceeding with pie-crusting of the MCL.
Pie-crusting of the MCL is performed percutaneously with a needle, and involves making multiple tiny perforations in the medial collateral ligament and mainly in the posterior oblique portion of the medial tissues. This is best done with the knee at about 20 degrees of flexion under a valgus force. As the medial tissues ‘give’ there is a palpable (and sometimes audible) tearing of the tissues and the medial compartment opens up further by just a few additional millimetres. This makes a massive difference and allows radically improved visualisation and access to the whole of the posterior portion of the medial compartment.
1. Tight medial compartment with poor and restricted view of the posterior horn of the medial meniscus.
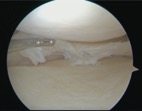
2. Significantly improved view and access to the posterior aspect of the medial compartment and the posterior horn of the medial meniscus after pie-crusting of the MCL (showing a far more extensive ragged degenerate meniscal tear compared to what was visualised initially, prior to pie-crusting).
If there is any kind of tear in the posterior horn of the medial meniscus, then this can then be seen, probed and dealt with far more easily and with a much lower risk of A) missing the true extent of a tear, B) missing a tear altogether, C) failing to deal fully and sufficiently with whatever tears might be present, or D) scuffing and damaging the articular cartilage on the surface of the medial femoral condyle by struggling to gain sufficient access. Once the MCL has been pie-crusted, it is then far easier to feel (with the arthroscopic probe) and actually see and then deal with a ramp lesion.
Research has shown that the MCL heals very well indeed after pie-crusting (just like a minor partial MCL tear / sprain), with no residual valgus laxity in the joint and with no adverse long-term sequelae. As stated above, the threshold for pie-crusting the MCL should be very low.
Ramp lesion repair
Once a ramp lesion has been identified, it is then relatively easy and straight forward to repair the tear, and this absolutely can be performed using an all-inside technique via standard anteromedial and anterolateral portals. However, what is required is an all-inside meniscal suturing device that is reliably bendable, which is where the Stryker AIR+ device really comes into its own.
The Stryker AIR+ meniscal repair device has a delivery needle that can be bent at its end by as much as 90 degrees. With this, multiple sutures can be placed through the tibial under-surface of the meniscus and down and backwards through the meniscotibial ligament, which is ideal for repairing a ramp lesion nice and securely.
Surgical video of a ramp lesion repair
Watch a video of the surgical technique for the repair of a medial meniscal ramp lesion using Stryker AIR+ meniscal repair sutures:
In conclusion
KEY POINTS
- Meniscal ramp lesions are a common finding in ACL-deficient knees.
- Ramp lesions can sometimes be seen on MRI, but are often missed.
- One should always have a very low index of suspicion for there potentially being a ramp lesion present in every ACL-deficient knee and at the time of every ACL reconstruction.
- Even with poor access, a ramp lesion can pretty much always be felt (even if not seen) with an arthroscopic probe from standard anterior portals.
- If a ramp lesion is even suspected, then one should have a very low threshold for pie-crusting the MCL if visualisation and access to the posterior aspect of the medial compartment are in any way suboptimal.
- One the MCL has been pie-crusted, it becomes easy to see and deal with tears in the posterior horn of the medial meniscus, including ramp lesions.
- If missed or left, ramp lesions can cause ongoing symptoms in the knee and can adversely affect the biomechanical function of the joint.
- Ramp lesions can be repaired with a relatively simple (if somewhat ‘fiddly’) all-inside technique via standard anteromedial and anterolateral arthroscopy portals, with an ‘all-inside’ meniscal repair device that is bendable: i.e. the Stryker AIR+.
