
#condition
Locked Knees
KEY POINTS:
- A locked knee = a displaced locked bucket handle meniscal tear, until proven otherwise.
- A patient with a locked knee needs an MRI scan within a few days, not weeks.
- If there is a bucket handle meniscal tear, then this needs arthroscopic (keyhole) surgery urgently: i.e. ideally within days, or a week or so at most.
- If a displaced locked bucket handle tear of a meniscus is caught early (within the 1st 6 weeks or so), then it may be reducible and repairable, in which case the meniscus can then be salvaged.
- If a displaced locked bucket handle meniscal tear is left too long (more than about 6 weeks), then it is almost never reducible or repairable, which means that the bucket handle fragment will end up having to be removed. This normally means a subtotal or even total meniscectomy, which then very significantly increases the long-term risk of future arthritis in that knee.
Therefore:
- A locked knee needs urgent referral for an MRI scan,
- and it is likely to need urgent arthroscopic knee surgery.
- DO NOT try and treat this conservatively, and
- DO NOT delay referral to a knee specialist.
The term ‘locked knee’ is used to refer to a knee where something ‘happens’ and where someone finds that they can then no longer fully extend (straighten) their knee.
If someone just gradually develops stiffness in a knee that is painful and swollen, and if the knee gradually deteriorates with time so that one can no longer fully straighten the joint, then this is not a locked knee: instead, this is referred to as ‘a fixed flexion deformity’, which is a sign of progressive knee arthritis.
A locked knee, by comparison, is where someone’s knee was normal (or close to normal) but then there is specific trauma (e.g. twisting on a bent knee) or a specific ‘event’ (e.g. the knee suddenly gets stuck when one is getting up from squatting / kneeling / sitting cross-legged), and there is sudden pain and an inability to fully straighten the joint.
Sometimes the knee may stay locked – which is when the situation is then urgent. Sometimes, however, the knee may ‘unlock’, and it may potentially do so with a clunk or a click, with sudden brief pain but with the knee then feeling noticeably better afterwards.
There are a number of specific things that can cause a knee to lock, and these include:
- a displaced locked bucket handle meniscal tear,
- a tear of the ACL (the anterior cruciate ligament),
- a loose body within the joint or
- an unstable lateral meniscus (specifically, instability/hypermobility of the posterior horn of the lateral meniscus.
The displaced locked bucket handle meniscal tear
There are two C-shaped wedges of elastic cartilage in each knee joint: one on the inner side of the knee, called the medial meniscus, and one on the outer side, called the lateral meniscus, and these act as load sharers / ‘shock absorbers’ within the knee. The meniscal cartilages can, and often do tear. If there is a large tear around the circumference of a meniscus then the inner portion can become unstable. This inner ‘bucket handle’ section of the meniscus can sometimes flip over so that a chunk of meniscus is sitting right in the centre of the middle of the knee instead of around the edge of the joint. This displaced tissue gets jammed in the wrong place inside the knee and causes a mechanical block, preventing full extension.
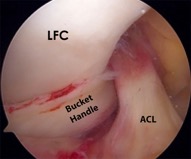
Displaced locked bucket handle tear of lateral meniscus causing locked knee.
Importantly:
A locked knee = a displaced locked bucket handle meniscal tear until proven otherwise!
If a displaced locked bucket handle meniscal tear is caught early, which means within the first 6 weeks or so, then it is often possible to reduce the displaced fragment back into its proper place and to repair it, with multiple meniscal stitches. This then has a very good chance (up to about 90%) of healing successfully, in which case (after appropriately slow and careful rehab) the knee then tends to get back to normal (or at least fairly close to normal).
If a displaced locked bucket handle meniscal tear is left, then with time the bucket handle fragment will scar up and contract, so that it becomes increasingly difficult, or eventually impossible to surgically reduce the fragment back in place. Also, the longer the bucket handle meniscal fragment is left in a displaced position, the more it will get ground down and damaged by repeated movement and loading of the knee. If a bucket handle meniscal fragment is irreducible or if it is too badly damaged (frayed / ragged), then it becomes impossible to reduce and repair the meniscus. If this happens, then the meniscal fragment will end up having to be removed from the knee. Importantly, most bucket handle tears occur around or towards the peripheral edge of the meniscus and they tend to involve a majority, if not all of the volume of the meniscus. Therefore, if the meniscal fragment does end up having to be removed from the knee, then this normally means loss of most, if not all of the meniscus.
The meniscal cartilages in the knee are extremely important structures, with multiple functions, but with their prime function being as load sharers. If a meniscus ends up having to be removed from a knee (a meniscectomy) then this massively increases the risk of future arthritis in that compartment (side) of the knee in the future:
Loss of a meniscus increases the risk of you developing knee arthritis
within the following 20 years by x 15 (i.e. a 1500% increased risk).
Therefore, all reasonable attempts should be made to preserve the meniscal cartilages wherever possible… and the best way to ensure that a displaced locked bucket handle meniscal tear can be reduced and repaired, and therefore saved, is to identify it ASAP and, where appropriate, to operate ASAP.
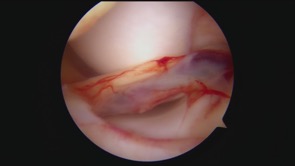
Arthroscopic view of the front of a left knee with a displaced locked bucket handle tear of the medial meniscus, with a locked knee.

Bucket handle ‘fragment’ of the meniscus (actually = the full width of the whole meniscus) reduced back into place.

Meniscus repaired with multiple sutures, giving a stable result and preserving the whole meniscus.
The locked / pseudolocked knee with an ACL tear
If one tears the ACL in one’s knee, then this normally occurs from significant twisting-type trauma, such as a football tackle, a ski injury or a fall. Sometimes, the torn stump of the ligament can sit at the front of the knee and it can get ‘pinched’ at the front of the joint in extension, which means that it’s then painful to straighten the knee.

MRI scan showing a torn ACL stump sitting trapped at the front of the notch.
The stump of a torn ACL may cause a physical block (i.e. an actual locked knee) or it may simply cause ‘apparent’ locking, where the inability to fully extend the knee is caused by pain from the torn ACL stump being ‘pinched’ at the front of the knee in extension. This latter situation is what is referred to as ‘pseudolocking’, meaning that the knee seems to be locked, but this is actually due to pain inhibition – and therefore, if one were to give an anaesthetic or just leave the knee alone and give it time to settle down, then the joint would normally tend to straighten out fully.
Importantly, even if a patient has a history and clinical examination findings suggestive of an ACL tear, it is still vital to get an urgent MRI scan to check exactly what damage there might be inside the knee: importantly, displaced locked bucket handle meniscal tears can also occur in a knee along with a tear of the ACL, simultaneously.
Lateral meniscal instability
The medial and lateral meniscal cartilages are slightly different shapes from each other plus they also have slightly different attachments holding them in place. In particular, the posterior horn (the back portion) of the lateral meniscus is less firmly attached to the tibia, and there is a gap in the meniscotibial attachment called the popliteus hiatus (which is where the popliteus tendon sits). In some people the meniscotibial attachment at the back of the lateral meniscus can be very flimsy (especially in people with hypermobility and/or collagen disorders), and/or the attachment may tear from trauma (mainly from twisting on a bent knee). This can sometimes lead to the posterior horn of the lateral meniscus flipping forwards into the lateral compartment in deep flexion (when bending the knee) and causing locking, with a ‘clunking’ sensation in the knee. More often than not, this locking tends to be temporary and intermittent, with a feeling of discomfort around the lateral (outer) side of the knee. Lateral meniscal instability can also occur if the lateral meniscus is discoid: i.e. if you are born with a larger chunkier disc-shaped meniscus instead of a normal C-shaped meniscus (and this occurs in maybe 1.5% or so of the population).
One of the real difficulties in diagnosing lateral meniscal instability is that the lateral meniscus will, more often than not, tend to look normal on an MRI scan unless the meniscus is actually displaced / dislocated / subluxed at the time of the actual scan, which would be relatively rare. It is still essential to get an MRI scan to check for other potential intra-articular pathology; however, definite diagnosis is arthroscopically, via keyhole surgery, where the posterior horn of the lateral meniscus can be hooked with a probe and displaced anteriorly into the lateral compartment.
Posterior horn of a lateral meniscus displaced anteriorly in the lateral compartment and locked.
If suspected lateral meniscal instability is confirmed at the time of a knee arthroscopy, then the meniscus can usually be fixed back in place with multiple meniscal stitches, all inserted arthroscopically (via keyhole surgery). More difficult cases, where a previous attempted arthroscopic repair has failed and/or where the patient has a collagen disorder may require more extensive/invasive surgery, with an open meniscal repair: thankfully, however, this is only rarely ever required.
IN CONCLUSION
- A locked knee should be investigated with an urgent MRI scan – within a few days, not weeks or months.
- A locked knee = a displaced locked bucket handle meniscal tear…. until proven otherwise.
- A displaced locked bucket handle meniscal tear should be treated surgically, with either an arthroscopic (keyhole) meniscal repair, if possible, or else an arthroscopic meniscectomy (removal), if necessary, and the surgery should be performed urgently – i.e. within a few days, if possible, or else within a week or two at most.
- Any patient with a locked knee should be referred urgently to a Consultant Orthopaedic Surgeon specialising in knees, who can see, investigate and appropriately treat the patient as an urgent priority.
